
GERIATRIC NUTRITION, A FUNCTIONAL PERSPECTIVE: WHAT TO EAT TO AGE WISHFULLY
Protein is mainly sourced from animal products like meat, fish, poultry, and dairy products. Beans, legumes, and certain grains contain them too, but not in high or concentrated amounts. We often require a combination of more significant amounts of these plant foods to hit protein goals than if we were to simply take in a portion of meat, poultry, or fish. This often requires a large amount of food to be consumed to achieve protein guidelines.
Because of many recent movements demonizing red meat and animal products as a whole, we've seen many people move away from consuming animal products and a decrease in overall protein intake. When we're not consuming animal products containing protein, we're also not getting a wide array of micronutrients as vitamins and minerals in high enough concentrations or in available forms that are critical for survival. As a result, we end up micronutrient and macronutrient deficient. While we may not see the ill effects immediately, health ailments of the elderly tend to be a result of repeated deficiency over time that has accumulated.
Biochemistry has shown us that protein-rich foods like poultry, beef, lamb, pork, fish, and dairy products are the only bioavailable sources of:
Vitamin A (retinol) - Vitamin A in its retinol form is critical for the immune system, eye health, and the integrity of mucosal membranes of the gastrointestinal and respiratory systems. Beta carotene is the provitamin form of vitamin A that requires an additional conversion that is inefficient in humans.
B Vitamins (specifically B12) - B12 is critical for memory, energy production, the health of nerves, and many other functions. B12 is not found amply in non-animal foods.
Iron (Heme) - Non-heme iron is found in plant foods, but it's known to be absorbed poorly. Iron is needed for memory, energy function, synthesis of red blood cells, and oxygen transport.
Calcium - Although calcium is found in some plant foods, it is arguably poorly absorbed. Calcium is extremely important for strong bones, nerve function, and the health of the central nervous system.
Zinc - Although zinc is found in many plant foods, it is difficult to absorb from them because of phytates in foods that can hinder its absorption. Zinc is needed for immune function, stomach acid production, healthy mood, hormone synthesis, and the health of the nervous system.
Omega-3 Fatty Acids - Omega-3s in their bioavailable EPA and DHA forms are not found readily and amply in plant foods. These are critical for a healthy brain as much of the brain is made of fats. They are also essential for memory, mood, and inflammation.
When we "eat protein" in the form of animal products, we are not just eating protein. We are consuming the valuable micronutrients alongside it that are not found in other plant foods. As a result, if we are NOT eating protein regularly, it's rather hard to get these crucial micronutrients in their most bioavailable forms that have such vital roles in the nervous system—especially in those who are aging!
DAIRY
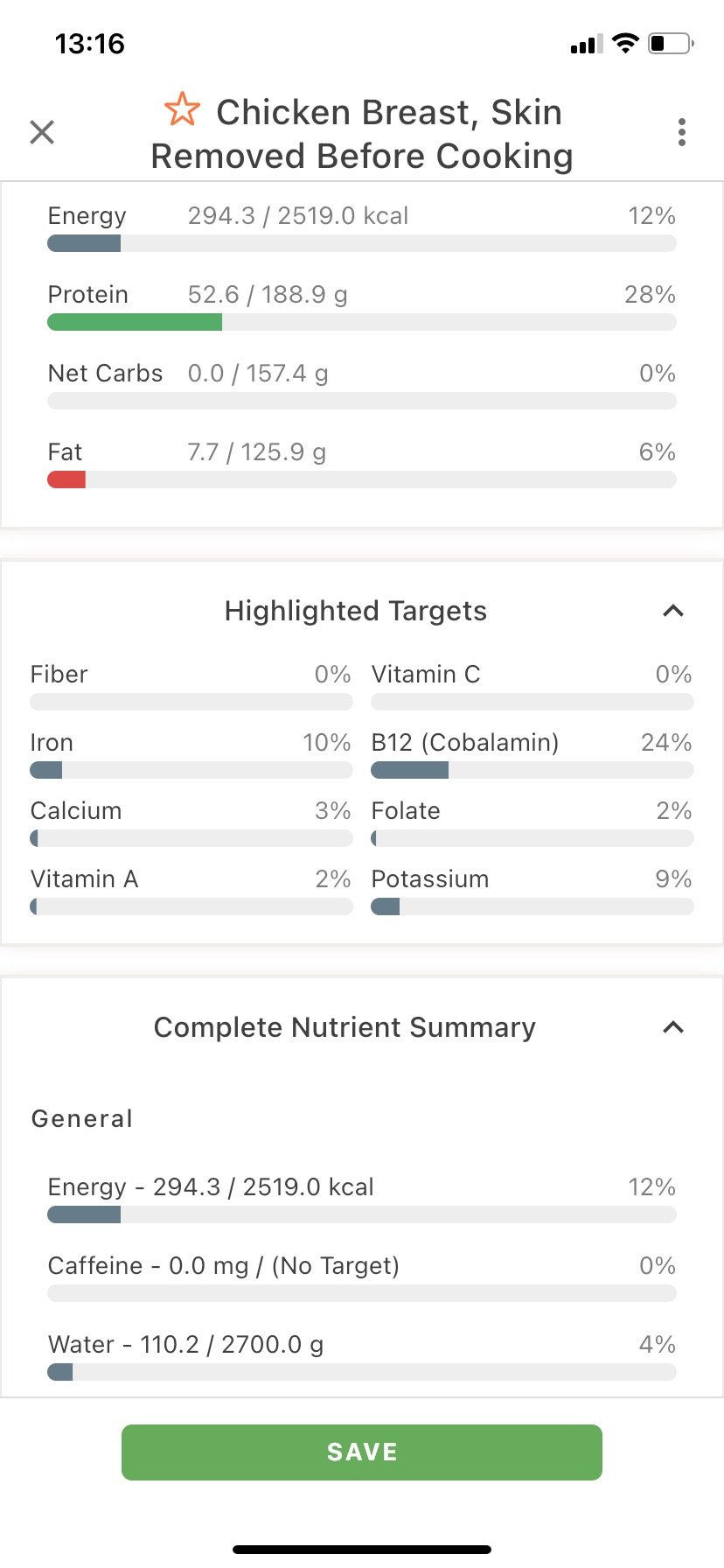
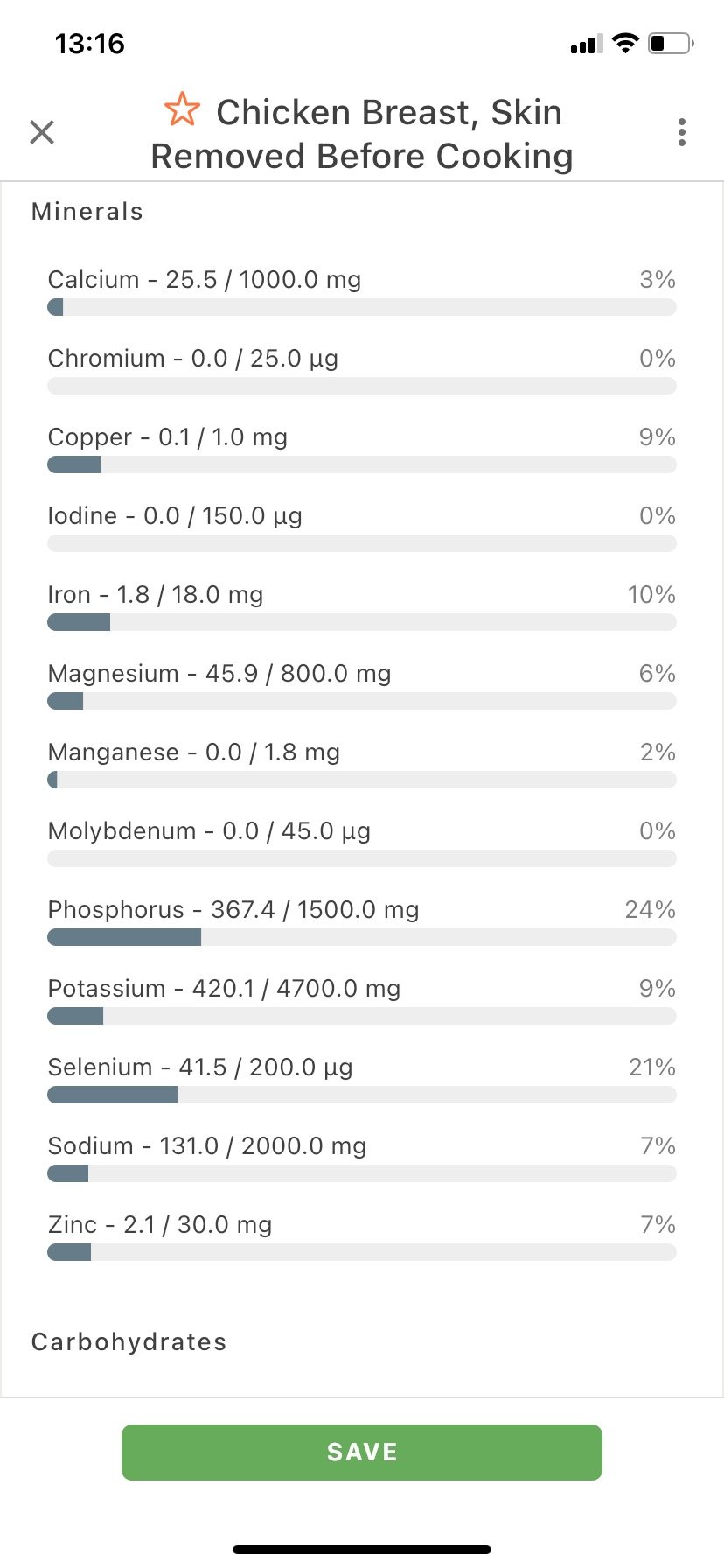
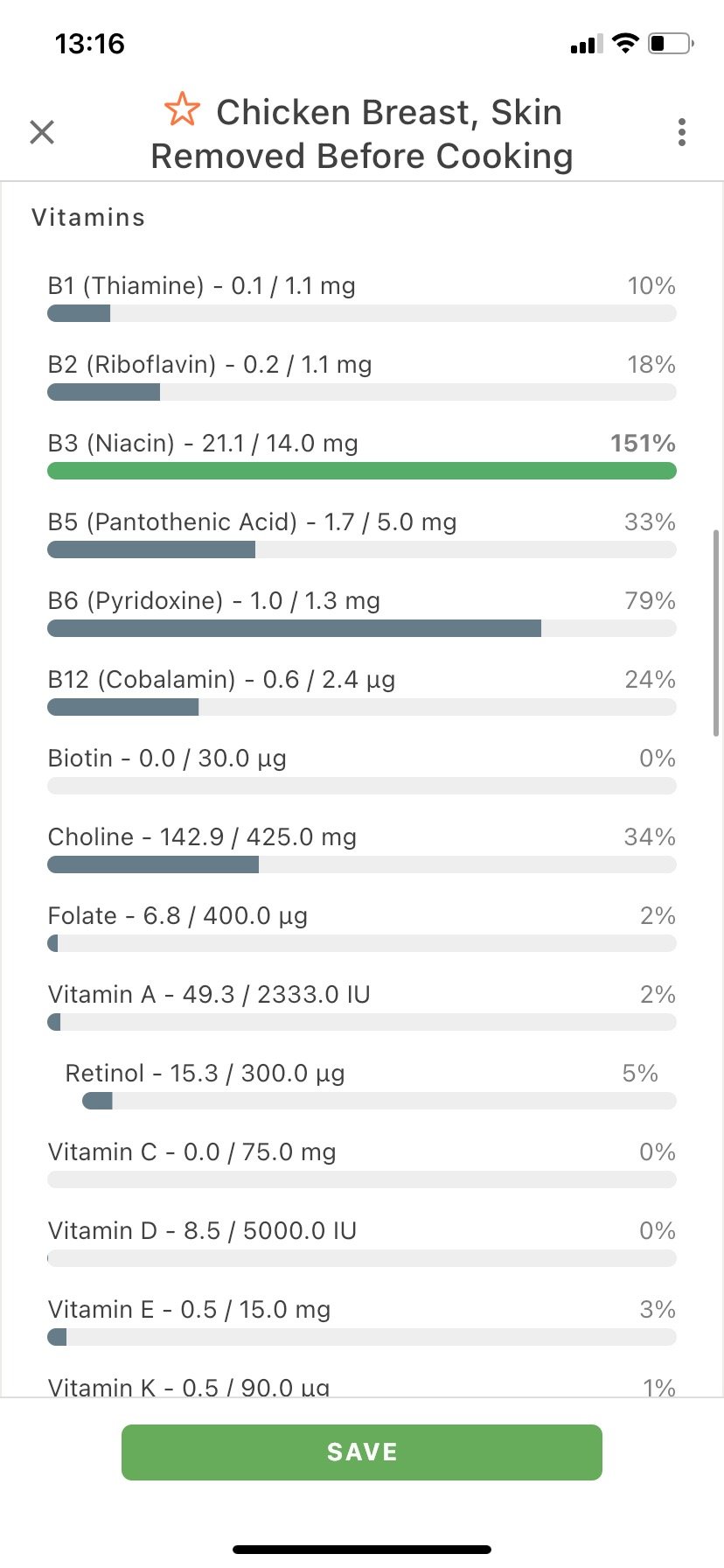
While dairy isn't a macronutrient, it possesses something that no other macronutrient can: calcium in a bioavailable form. The "Got Milk?" Campaign of the early 2000s had its benefits, and I'd argue that it's a detriment that it dropped off—minus promoting industrialized dairy farming. The current recommended daily intake for calcium sits somewhere around three cups, which is arguably even low. However, most seniors struggle to hit only one. I've included a Cronometer estimate of what "one cup" of reduced-fat milk looks like in terms of micronutrients and macronutrients.
GERIATRIC NUTRITION
The other night, I spoke with one of my close friends who has been spending a lot of time with her grandparents on the East coast. We talked tangibly about nutrition, and she briefly mentioned some of her grandfather's diet habits that he was incorporating. She also said that since being around them more, she hadn't come across any well-versed geriatric nutrition advice that wasn't touting mainstream USDA recommendations. I did some research, and I couldn't find much either. I find this to be somewhat of a crime.
Our 65+ population has given us life. However, they're falling victim to conditions like diabetes, osteoporosis, muscle wasting (sarcopenia), heart disease, and neurodegeneration that—in my opinion—are very preventable. Considering my mom turns sixty-five this year, I woke up this morning motivated to write an introductory blog on senior (geriatric) nutrition and my functional perspectives on the subject.
This blog will cover WHY a problem exists and WHAT some of the current recommendations are. We will then move into WHAT the problem is with current guidelines and HOW these same guidelines may contribute to some conditions that regularly plague our elders. Let's begin!

LIKE 400 WORDS TO COVER 200000 YEARS
Mainstream nutrition leads us to believe that there is one finite lens to look through to lead a healthy life. It does not.
I believe everyone reading this article has the intelligence and aptitude for discerning which diet they believe is the best for them based on how they feel unless they're following a diet specific to a condition, like adhering to a therapeutic ketogenic diet for cancer. No doctor can tell someone what it truly feels like to be in their body... especially with generalized nutrition guidelines. Only you and your actions can.
The intervention of science, modern industry, and agriculture all have come to collide with innate wisdom. What once was nutrition guided by evolution now has colluded with too many conflicts of interest. As a result, our dietary recommendations might be considered unnatural and may contribute to the very diseases they're claiming to prevent.
For thousands of years, anthropology, history, and archaeology have shown that we as humans evolved as hunter-gatherers. We migrated to follow our prey. With the incorporation and development of agriculture and farming coming into the picture about twelve thousand years ago, foods like grains were not staples in our diets until only a relatively short time ago. While grains at this time were undoubtedly more nutrient-dense than those we see today, they were far different in terms of any "staple" we'd previously fixed our plates on.
Around four hundred years ago, the amount of white sugar that humans consumed increased substantially with slavery and trading. Foods with this new addictive addition had never been so readily available before, nor had sugar been so amply available. As the demand increased, production increased. Profit from this new commodity also was on the rise.
Industrialized farming—known commonly as "big ag"—took to producing large amounts of cheap crops like soy, corn, and wheat that called on a lot of inexpensive and—at the time—plentiful resources like fossil fuels, pesticides, and land. Pharmaceutical companies got involved by tailoring studies to support products that they produced. Food companies grew bigger and richer as these "tasty" foods were more plentiful and supposedly healthier.
Over one hundred years ago, the industrialization of food production took off. We discovered flavorings, preservatives, and processes like hydrogenation. This combined all aspects of hyper-palatability into foods we know today as "junk": sugar, white flour, and processed fat.
Marketers quickly took to selling these new "drugs" to the population. Once it was realized that profit could be made from such hyper-palatable foods, it wasn't long before other high-profiting industries, including the pharmaceutical and agricultural sectors, got involved.
Some of you may know the correlations between the industrialized food industry, and others may not. But for those of you who are new here, there are some conflicts of interest. For example:
Almost all fast-food, junk food, and commercial home products can be traced back to ten manufacturers. Some of these manufacturers also have direct and indirect links to the big farm companies like Cargill and Monsanto and pharmaceutical companies like Pfizer and Johnson & Johnson.

Certain drug companies also make food products. A good example is Johnson and Johnson making drugs and producing the controversial sweetener Splenda shown to have health implications.
Published scientific studies are regularly complicated with conflicts of interest. Industrial food manufacturers and producers use their influence with the health sciences to produce favorable research to sell products.

They also use their research to make foods look less favorable.

You can read a bit more about these "coincidental" studies here: https://www.foodpolitics.com.
Industrialized food manufacturers, pharmaceutical companies, and large-scale agricultural companies expend the most money to influence legislation in the U.S., and other nations.
This section warrants a blog post of its own. My point is not to denounce capitalism but to show how all influence one another to make a profit. We will get into how that has influenced your health now.
CURRENT DIETARY RECOMMENDATIONS FOR 65+
The next stop on my research train was to see what is being recommended by doctors and nutrition professionals. Coming from a background of functional nutrition, I will admit that I hadn't checked senior guidelines per the USDA before today. They had me a bit confused. I've pulled some of the graphics from the U.S. dietary guidelines straight from their website to talk and review.

PROTEIN
Protein is one of three dietary macronutrients that we get energy (calories) from. Protein is our only dietary source of complete amino acids. Amino acids help to make up and carry out every biological process! Protein and associated amino acids do it all, whether it be tissue repair, enzyme synthesis, or DNA and RNA repair.
We will discuss just how low protein intake can contribute to many illnesses plaguing the elderly, but I wanted to first draw attention to how most are only actually taking in around 5-6 ounces of protein per day. That's a measly fifty-six grams of protein, which equates to approximately only three hundred calories or less than ten percent of what most should be taking in from calories! This recommendation just hits WHO baseline guidelines for essentially escaping starvation. Unfortunately, consumers aren't even advised to take in much more.
We will discuss just how low protein intake can contribute to many illnesses plaguing the elderly, but I wanted to first draw attention to how most are only actually taking in around 5-6 ounces of protein per day. That's a measly fifty-six grams of protein, which equates to approximately only three hundred calories or less than ten percent of what most should be taking in from calories! This recommendation just hits WHO baseline guidelines for essentially escaping starvation. Unfortunately, consumers aren't even advised to take in much more.
Protein is mainly sourced from animal products like meat, fish, poultry, and dairy products. Beans, legumes, and certain grains contain them too, but not in high or concentrated amounts. We often require a combination of more significant amounts of these plant foods to hit protein goals than if we were to simply take in a portion of meat, poultry, or fish. This often requires a large amount of food to be consumed to achieve protein guidelines.
Because of many recent movements demonizing red meat and animal products as a whole, we've seen many people move away from consuming animal products and a decrease in overall protein intake. When we're not consuming animal products containing protein, we're also not getting a wide array of micronutrients as vitamins and minerals in high enough concentrations or in available forms that are critical for survival. As a result, we end up micronutrient and macronutrient deficient. While we may not see the ill effects immediately, health ailments of the elderly tend to be a result of repeated deficiency over time that has accumulated.
Biochemistry has shown us that protein-rich foods like poultry, beef, lamb, pork, fish, and dairy products are the only bioavailable sources of:
Vitamin A (retinol) - Vitamin A in its retinol form is critical for the immune system, eye health, and the integrity of mucosal membranes of the gastrointestinal and respiratory systems. Beta carotene is the provitamin form of vitamin A that requires an additional conversion that is inefficient in humans.
Cobalamin (B12) - B12 is critical for memory, energy production, the health of nerves, and many other functions. B12 is not found amply in non-animal foods.
Iron (Heme) - Non-heme iron is found in plant foods, but it's known to be absorbed poorly. Iron is needed for memory, energy function, synthesis of red blood cells, and oxygen transport.
Calcium - Although calcium is found in some plant foods, it is arguably poorly absorbed. Calcium is extremely important for strong bones, nerve function, and the health of the central nervous system.
Zinc - Although zinc is found in many plant foods, it is difficult to absorb from them because of phytates in foods that can hinder its absorption. Zinc is needed for immune function, stomach acid production, healthy mood, hormone synthesis, and the health of the nervous system.
Omega-3 Fatty Acids - Omega-3s in their bioavailable EPA and DHA forms are not found readily and amply in plant foods. These are critical for a healthy brain as much of the brain is made of fats. They are also essential for memory, mood, and inflammation.
When we "eat protein" in the form of animal products, we are not just eating protein. We are consuming the valuable micronutrients alongside it that are not found in other plant foods. As a result, if we are NOT eating protein regularly, it's rather hard to get these crucial micronutrients in their most bioavailable forms that have such vital roles in the nervous system—especially in those who are aging!
DAIRY
While dairy isn't a macronutrient, it possesses something that no other macronutrient can: calcium in a bioavailable form. The "Got Milk?" Campaign of the early 2000s had its benefits, and I'd argue that it's a detriment that it dropped off—minus promoting industrialized dairy farming. The current recommended daily intake for calcium sits somewhere around three cups, which is arguably even low. However, most seniors struggle to hit only one. I've included a Cronometer estimate of what "one cup" of reduced-fat milk looks like in terms of micronutrients and macronutrients.
While calcium isn't the only player in terms of bone health, it's a big part of it. Milk is also one of the few foods that contain vitamin D, which is crucial to absorbing calcium in the digestive tract.
Calcium deficiency can have dire consequences on a population prone to osteoporosis, osteopenia, and injuries from falls. What's worse? It's often recommended to consume low-fat dairy, which—as we will see—also isn't as healthy as we're led to believe.
FATS
Fats and their respective recommended intakes are widely debated in all generations of health and nutrition. I would argue that the elderly population is specifically more resistant to taking in dietary fat because of nutrition information that they've been exposed to from a young age.
When Dwight D. Eisenhower was in office, there was a significant shift in dietary recommendations following his much-publicized stroke and with Ancel Keys' "revolutionary" studies on saturated fat. Much of Ancel Keys' work has long been under scrutiny and has been questioned for some of its flaws. We will examine some of them and how these shortcomings have since been supported with updated science.

Fat Hatred History
The 1950s were a time when rates of cardiovascular disease were SOARING. Given the high prevalence of stress following World War II, a depression that had influenced the population for only a decade or so before, an over-motivated work culture, and rampant alcohol and smoking, it's no shock heart attack rates were so high during this time! Processed foods were relatively new in the diet, and most were still only allotted on occasion. Despite these factors, we took to only looking at the same food we'd been consuming for millennia, like meat, dairy, and saturated fat from foods like butter.
With Eisenhower's stroke, a man named Ancel Keys took to performing his "Seven Countries" Study to examine the role of lifestyle factors in cardiovascular disease in varying nations like the U.S., Northern Europe (Scandinavia), Greece, Yugoslavia, and Japan. He used his findings to "prove" that diets rich in animal fats correlated to high blood cholesterol levels and that high blood cholesterol levels were linked to higher incidences of all-cause mortality and heart disease in western nations. It did not examine other possible causes of CVD, like stress, alcohol, smoking, and other potential links like environmental toxins—all very prevalent in these nations, especially following WWII!
Despite all of Keys' studies "pointing" towards animal fats caused disease, he could never disprove "The French Paradox", "The Spanish Paradox", or other "paradoxes" of similar European nations that had clean bills of cardiovascular health despite increased saturated fat intake. They were simply reported in findings as "such and such paradox". Boring from a country where we are "innocent until proven guilty," it's often been questioned by professionals why Mr. Keys was not more curious about his contradictory findings. It was later pointed out that Mr. Keys had neglected to include all research on the actual twenty-one countries he conducted studies on. Attention was also brought to Mr. Keys' neglect in discussing the effects of trans fatty acids and sugar on health.
With the studies done by Mr. Keys, the industrialized food industry had precedence over marketing some of its newly processed "heart-healthy" foods, like plant oils and grain products, which we'll talk about later. Plant oils like canola, soybean, sunflower, safflower, corn, vegetable, and cottonseed oils have since been linked to higher incidences of inflammation, diabetes, insulin resistance, and conditions like non-alcoholic fatty liver disease (NAFLD). To think that foods we evolved to eat like meat and our own breast milk are superseded by synthetic, industrialized oils that are processed from raw ingredients that aren't indigenous to the human diet seems pretty bizarre when you think about it… doesn't it?
If you're interested in learning more about how our perspectives on saturated fats changed throughout history, The Big Fat Surprise by Nina Teicholz is a great read. It was written after nine years' worth of investigative journalism on the subject and will likely leave you questioning things.
Dietary Fat and Cholesterol: Is There A Link?
If you ask most doctors if there is a link between dietary fat and high cholesterol, they'll tell you that "yes, it does" without a blink of an eye. If you open up any introductory level biochemistry book—a foundational study in medicine—you will get an answer that contradicts their response.
We need cholesterol for many life processes. Without it, we would simply break down and die. We need cholesterol to make cell membranes, for example. We also need it to make steroid hormones like our sex hormones and the infamous stress hormone cortisol. When cholesterol is reduced in the human body, like with statin drugs, there are known detriments like aggression and changes in demeanor from its effects on hormone synthesis.
To keep it short and sweet: there is a link between dietary cholesterol and blood cholesterol, but it is not as proportional or finite as we've been led to believe. Eating fat does not simply mean our blood fats climb, climb, and climb; instead, only about ten to fifteen percent of the cholesterol in our systems comes from the food we eat. The liver synthesizes the organic molecule we know as cholesterol independent of if we get it in the diet. Based on the levels of free-circulating cholesterol in the blood, cholesterol production in the liver increases if we need more or decreases if we have enough.
Studies have shown that the real cause of increased blood cholesterol is linked to what we know today as insulin resistance. This, in turn, contributes to a decreased absorption of blood cholesterol by cells. What foods exactly contribute to insulin resistance remains debated in the nutrition world, whether it be fats, processed fats, carbohydrates in their entirety, or if it's from the very synthetic foods that are often recommended because of how their toxic additives disrupt metabolism. I'll hopefully do more on this last point in a future post :-).
Land O' Lakes is Land O' Fakes
My baba (grandma) bought into the vegetable oil train, but she never would touch margarine. Despite having multiple heart conditions, she talked about it like it was a disgrace. The labels had always read "heart-healthy" and "AHA approved," and I had always trusted it. When I began to take chemistry courses in high school and college, I started to question things after learning about hydrogenation.
To get why margarine is inferior to butter, we have to understand how it's made. Margarine is often a product of highly processed polyunsaturated fats, like canola, soybean, and sunflower oils. These fats are usually a liquid at room temperature because of the bonding structure between their carbon atoms: they are polyunsaturated or have several carbon-carbon bonds that are not saturated.
To turn these oils into margarine, they are subject to a process known as hydrogenation to saturate these bonds synthetically. Powdered mineral catalysts like potentially-toxic nickel or other metals are then added to a dissolved alkene and ethanol. They're next pressurized and heated to very high temperatures. The end product gives us Crisco or something similar to butter, but not butter (hence the "I Can't Believe it's Not Butter") and all of the trans fatty acids! These synthetic "trans fats" are known to contribute to diabetes, inflammation, and heart detriments on their own.
An interesting note on hydrogenation: this process was patented in 1908 by Procter & Gamble: one of the world's largest manufacturing companies that have taken to making some pretty popular drugs like the well-known Prilosec. This medication is regularly taken to alleviate heartburn that frequently accompanies high-fat, deep-fried meals.
But Back to Fats…
Currently, it's recommended for those who are 51+ to consume between 20-35% of calories from fats. This is merely forty-five grams of fat per day, or two teaspoons (yes, TEAspoon, I didn't miswrite that) of butter per meal. As we mentioned earlier, fats are needed for so many aspects of health. Our brains are around sixty-percent fat. Our hormones come from fat. We need hormones to regulate bone health. We absorb critical fat-soluble vitamins because of fat intake. We make vitamin D from dietary cholesterol reacting in our skin with sunlight. Fat is rather essential!
There is a condition known as "rabbit starvation" that results from the absence of fat in the diet. If someone is purely consuming no fat while consuming all of their calories from protein and carbohydrates, they eventually will starve to death because of the lack of lipids they're taking in. Fat has such a massive component to health, and our brains are wired to crave them for a reason. Fearing and avoiding them has arguably led to its own detriments!
Carbohydrates
With so little focus on protein and fat, you must wonder: what are we left to recommend our seniors eat?
U.S. Dietary Guidelines recommend a staggering forty-five to sixty-five percent of calories from carbohydrates. Carbohydrates make up our third macronutrient category. Carbs consist of fruits, vegetables, beans, legumes, grains, and all derivatives. We can also divide them into starches, sugars, and fiber. This number, to me, is staggeringly high. Why? Well, repeated studies have shown that fats and specifically protein contribute the most to satiation. Carbohydrates also tend to fluctuate blood sugar more than the other two macronutrients. However, this often depends on the type of carbohydrate, the quantity they're taking in of the carb, and the state of someone's metabolic health. Nonetheless… sixty-five percent of calories from carbohydrates is INSANELY high!
Looking at where the U.S. Dietary guidelines are allocating their carbohydrate recommendations, only around two to three cups are recommended to be taken in through vegetables per day. Only two cups of fruits (again, per day) are recommended to be taken in the form of carbohydrates.

While this might seem like a lot, this doesn't transfer much to make a dent in that forty-five percent (900 calories) to sixty-five (1300 calories) percent of calories from total carbohydrates.
If we'd like to use an example here, if we get our two cups of fruit from:
one cup of pineapple (24 kcal) and
one cup of apples (25 kcal)
and our vegetables from:
One cup potato (220 kcal)
One cup mixed vegetables (25 kcal) and
One cop of mushrooms (28 kcal)
… we've barely hit 350 kcal from carbohydrates!
So, where does the USDA expect us to hit our carbohydrate goals (and inherently the remaining ~50% of our caloric goals)?
Grains.

Grains
Grains are something I go back and forth with that I'd love to leave for discussion on a future blog, but let's be honest: however long that might be from now, given my track record, I don't know. In short, grains have only made it into our diet in the last ten to twelve thousand years with the introduction of farming, as we discussed early on. Once we learned how to domesticate agriculture, we shifted away from a "hunter-gatherer" lifestyle and more towards one centric around stationary farming. We could store and dry grains for the winter, and we could subside on things other than meats n' scavenged weeds. It was arguably a step forward for our species in many ways until the industrialized food industry took advantage of us.
Industrialized grains look like:
Cereals
Pasta
White flour
Granola bars
Chips (think Frito Lay)
Cookies
Crackers
Biscuits
Anything containing corn, soy, wheat, or derivatives
Sweeteners used in soda pops (Coke, Pepsi, A&W)
Candy
Fast-food products (KFC, Taco Bell, A&W), McDonald's, Burger King)
If we can go back to the corporation web we looked at earlier, we can see that most of these foods are produced by corporations linked directly or indirectly to other companies that benefit from you eating these foods.
These foods are "quick-sugars" that often spike blood sugar very rapidly and leave it to fall not long after. This is because very little fiber, bran, or natural starch exists in these foods compared to their whole-grain forms, which helps to slow the absorption and assimilation of carbohydrates (like natural foods have). Their high sugar content can also lead to rapid spikes in dopamine, which leads to addiction, similar to how drugs do. Many of these foods incorporate those artificial fats we talked about earlier, and they have very little protein (if any).
Almost all of these carbohydrate sources have little natural micronutrient value. This is to say that they have a very sparse vitamin and mineral content from the ultra-processing they undergo. The vitamins and minerals they do contain are fortified, which can be hard to absorb for some. Some of the forms of vitamins and minerals like iron fortification can contribute to toxicity. Finally, synthetic vitamins and minerals aren't in natural proportions as they are in whole food sources, meaning they can contribute to deficiency or excess of others. This is a complex topic I'd like to save—yet again—for a future blog post. Main takeaway: consuming fortified foods is inferior to whole foods with naturally occurring minerals and vitamins!
Conclusive Review on USDA "Recommendations"
U.S. Dietary Recommendations are very low in protein and fats (specifically healthy ones) relative to carbohydrates. Whether it's by coincidence or to purposefully feed the pockets of the pharmaceutical and food industries, it seems these very dietary recommendations could be contributing to the onset of various conditions that seem to plague the elderly. I will explore these top five states and how nutrient deficiency can contribute to their onset below.
CONDITIONS AND THEIR RELATIONSHIP TO NUTRITION
SARCOPENIA

Sarcopenia refers to "the loss of skeletal muscle has and strength as a result of aging". There are several contributing factors to sarcopenia in the aging population that are not exclusive to nutrition, like reduced physical activity and testosterone production. I'd also argue these are from nutrient deficiencies, but I'm trying to keep it simple. When looking at sarcopenia from a nutrition perspective, protein deficiency and not meeting protein needs consistently can contribute to muscle wasting. Several studies have been performed to examine the correlation between protein deficiency and sarcopenia, showing that intake of "soy or casein protein supplements" was efficient in sarcopenia prevention. I'm 100% in support of more protein, but what happened to a steak?
OSTEOPOROSIS / OSTEOPENIA / FALL-PROVOKED INJURIES

Falls are a significant cause of complications in the elderly from internal bleeding or infection with a broken bone. It is not uncommon for falls to result in bone breaks because of a condition stemming from weakened bone density like osteoporosis or osteopenia. While many might have you believe that this is a natural result of aging, I'm here to tell you it's not.
Bone integrity and bone density are maintained in part by sex hormones like testosterone and estrogen. Yes, these "drop off" to a certain degree when we age, but not to the extent we've been led to believe. How do we maintain such steroid hormones? Protein, the intake of healthy fats (cholesterol), vitamins D and K, and minerals like magnesium, calcium, and zinc sure help! Unfortunately, almost none of these macro and micronutrients come from grains or processed foods. Corn flakes and Wheaties do not have many of these nutrients at all to keep you strong and mighty, contrary to what you may believe!
On another note: sunlight—a free micronutrient precursor that allows us to produce vitamin D—is not accounted for in most nursing homes. There is little regard for making time for sunlight exposure in warm or cool months, nor is there consideration given across the masses to hit (at least) the RDA. Vitamin D is needed for calcium absorption, for the functioning of the central nervous system, and for immunity.
ALZHEIMER'S / DEMENTIA

The Alzheimer's and dementia epidemics are affecting people younger and younger. While these conditions may have some genetic predispositions, just because you possess a gene does not mean it will come true. Your environment can be defined as your stress levels, diet, and toxin intake. It greatly influences whether or not a gene you possess will exhibit a condition like Alzheimer's. This is known as the study of epigenetics, and I've written a little about it here. With that being said, Alzheimer's and dementia are still very real, especially if you continue to eat low-protein, low-fat, high-carbohydrate preservative-laden, and toxin-rich foods that contribute to brain inflammation.
Many recent studies have shown a high correlation between diabetes and Alzheimers. Many experts have started to call Alzheimer's and Dementia "type 3 diabetes". The exact mechanisms between high blood sugar and neurodegeneration are still being studied. Still, it has been shown that the inflammation and oxidative damage that is known to result from chronically elevated blood sugar can result in damage that looks like beta plaques, tau proteins, and neuronal damage. The damage that has resulted from reactive oxygen species contained in toxic foods has also been blamed.
DIABETES

This one is a bit more clear-cut than the others that you may be familiar with. Diabetes is a condition diagnosed based on chronically high blood sugars. There are two forms of diabetes: type 1 (T1D) and type 2 (T2D). T1D results from an autoimmune disorder that destroys beta cells that produce insulin within the pancreas. As a result, the body loses its ability to produce insulin, and one has to inject synthetic, exogenous insulin to survive. T2D is acquired from a poor diet, and it's more our focus.
As mentioned in the carbohydrate section, when we're consuming a high percentage of our calories from low-fiber, low-starch, high-sugar carbohydrates, as is the case with industrialized and grain-based foods, our blood sugar can quickly rise. Once the pancreas produces insulin to compensate for this blood sugar spike, glucose often drops below "normal," causing us to have low blood sugar not long after. This causes us to eat more and inherently becomes a vicious cycle of:
hungry—>processed food consumption—>high blood sugar—>insulin compensates to drop blood sugar
AND (viciously) REPEAT!

This goes on for years and years unless someone becomes self-aware! The pancreas gets worn out over time from producing so much insulin, and the body loses its sensitivity to this hormone. As a result, blood sugar remains high, and the pancreas "burns out." We lose our responsiveness to this hormone, and we gain weight. In time, we see hyperglycemia, pre-diabetes, and T2D (in time).
I wrote an e-book for a company a few months ago looking at the actual cause behind T2D. My evidence from the research showed that it was not a diet of high-carbohydrate intake but instead the result of a diet high in metabolism-disrupting, toxin-containing high-carbohydrates. Our metabolism is catalyzed (jumpstarted) by various vitamins and minerals. When we have an excess of toxins and a deficiency of micronutrients in our diet, our metabolism can be inhibited by this unfavorable swap [SOURCE]. Again, more on that in a future post!
T2D is a significant contributor to complications in the elderly, as it can contribute to:
Skin conditions
Eye damage
Kidney disorders
Neuropathy
Loss of limbs
Hearing impairment
Limb dysfunction
Heightened risk of infection
Alzheimer's and dementia
And it's very manageable, despite what most "professionals" will tell you.
HEART DISEASE
Heart disease has many manifestations, from atherosclerosis, high blood pressure, stroke, arrhythmias, clotting disorders, heart failure, and heart attack. All are prevalent in the elderly, and all are profoundly correlated to nutrition.
It is no secret that high blood sugar and toxins can contribute to vascular damage. This, in time, can contribute to the formation of sclerotic plaques and the mobilization of cholesterol that the body uses to repair itself. Much like trying to fix a leak in a pipe, this "patching of a hole" can contribute to sclerotic plaques that can play a role in high blood pressure, blood clots, and atherosclerosis.
It is also no secret that dietary insufficiency can contribute to vascular insufficiency and dysfunction. Arrhythmias are characterized as irregular heartbeats and have been linked to deficiencies in the mineral magnesium . Nutrient deficiencies like B1 (thiamine) can contribute—if not be behind—conditions like congestive heart failure. Incidences of heart attacks were found to be greater in individuals with greater insufficiencies in magnesium, also. Deficiency in antioxidants and micronutrients and excess environmental toxins like heavy metals like cadmium, mercury, and lead from the diet can lead to an imbalance of oxidative stress and an increase in a vascular tendency towards disease.
The bottom line: high blood glucose and nutrient-poor dietary habits can ultimately contribute to cardiovascular disease and the risk of developing related conditions.
DOES YOUR DOC KNOW ENOUGH TO ADVISE ON NUTRITION?
At the time of this article, I am enrolled as a medical student. For that reason, I feel that I can honestly weigh in on whether or not I believe a doctor has precedence to weigh in on nutrition. My answer? In short, no.
Doctors today are required to take one class in nutrition in medical school. One. This course is basic nutrition, covering what someone going into a general biological science would and outlining what primary macronutrients are. Doctors are required to take biochemistry and organic chemistry, yes. But many dread the subject despite these subjects serving as the foundation for the basis of medicine. These are courses of preclinical years that most frown and look down upon, at least in my experience with my peers.
Outside of these "basic" courses a doctor has to take to fulfill prerequisites, there may be the opportunity to take basic nutrition electives, depending on your doctor's school. But this is the extent of nutrition education! If a doctor wants to educate on nutrition, they can do so on their own time, or they can wait to do research, complete a Ph.D. or an M.S. in nutrition upon finishing their M.D. With residency and the many years doctors have to put in to get to actual practice. This is hard to come by unless they did their undergrad in nutritional science, which is rare. What I'm saying is most doctors do not have much additional knowledge in the nutrition field than anyone taking an introductory biochemistry course. It's really not their fault!
Keep in mind: medicine is science, like chemistry, biology, or physics. Science is not medicine. Stop holding them to such high accords with what they're telling you to eat! I'm sure this will piss a lot of people off, but it needs to be said. It's part of why we're so fat and sick!
MY Geriatric Nutrition Two Cents
Keep in mind: the following information is merely my perspective on what could be more beneficial eating habits for the elderly population. This is not a post to diagnose, cure or treat, and please take this post as it is intedned: for perspective and educational purposes only. Please read my disclaimer at the bottom of my website and speak with your doctor before incorporating any recommendations. With that being said…
Protein

First and foremost, I believe most seniors would benefit from a stark increase in protein. We want to avoid catabolism that can contribute to sarcopenia, and we want to correct any mineral deficiencies that could contribute to bone disorders. We also want to increase our micronutrient intake and stabilize our blood sugar. Incorporating more protein seems like a perfect answer!
It may be helpful to consume a minimum of one hundred grams of protein (four-hundred calories) for females or one-hundred twenty grams of protein (four-hundred eighty calories) for males. If this seems like a random number, it's merely twenty-five percent of the recommended one-thousand six-hundred (female) and two-thousand calories (male) recommended to AT LEAST be consumed daily for seniors. There are no detriments to consuming more calories and more protein (both are encouraged more from me, anyway) unless there's a pre-existing condition in place. Of course, it is best to spread protein throughout the day.
This often looks like around four to six ounces of lean protein per meal. I've given a few examples of what specific forms of animal protein can look like to incorporate per meal:
5 oz. smoked salmon: 230 kcal, 30g protein
5 oz. cooked chicken breast: 230 kcal, 43g protein
Three eggs: 215 kcal, 19g protein
6 oz. 90% lean hamburger meat: 300 kcal, 34g protein
6 oz. sea bass: 164 kcal, 30g protein
Remember: animal protein also has a high density of micronutrients (vitamins and minerals) like heme iron, bioavailable omega-3 fatty acids, vitamin A in the form of retinol, zinc, and B12 that are pertinent for the health of the central nervous system, immunity, and for healthy hormones that regulate so many processes.
Fats

I realize it's going to be hard to unlearn several decades of being coerced to believe that polyunsaturated plant oils are a panacea, but take a look and tell me: before the 1950s when these oils picked up in prevalence, do you recall as many incidences of obesity, neurodegeneration, autoimmunity, autism (was practically nonexistent), cancer, Alzheimer's', dementia, or cardiovascular complications? I wasn't alive back then, but I can sure say that the pictures and disease reports say "no!". Having moved to Eastern Europe, I can also say that the higher intake of saturated fat and a lower intake of polyunsaturated fats has indeed made for a skinnier and healthier population than that of the U.S. Because dietary fats are so essential for the synthesis of hormones, the fluidity of our cell membranes, and for the health of our brains, I would recommend upping the intake of quality, natural, unprocessed fats. Lucky for you, this includes butter!
I firmly believe that fats and carbohydrates should adjuncts next to protein to fill energy demands. Protein should be prioritized, with fats and carbohydrates being used as "levers" in balance unless a metabolic or neurodegenerative disorder needs to be catered to adjust based on caloric demands. While USDA guidelines recommend a measly ten percent of calories from fats, I would recommend experimenting with between thirty and fifty percent of calories from fats to fulfill dietary requirements.
For a male consuming 2,000 calories, this looks like anywhere between six hundred to one-thousand calories from fat, or anywhere from 66 to 111 grams of fat. For a female consuming 1,600 calories, this looks like anywhere between 53 and 89 grams of fat. Again, these are general caloric recommendations that I have tailored macronutrient ratios to. You or your loved one may differ in your caloric demands based on activity or if you have a disorder affecting metabolism.
Healthy fats come in many forms. Monounsaturated fats come from olive oil, avocados, and avocado oil. Polyunsaturated fats are sourced from nuts, seeds, and cold-water fish like salmon, mackerel, herring, sardines, and anchovies. Saturated fat is found in beef, lamb, pork, poultry, dairy, and coconut oil.
Fats to AVOID include sunflower, safflower, canola, soybean, peanut, rapeseed, grapeseed, vegetable oil, vegetable shortening, and margarine. I would also avoid cooking on high heat with any nut or seed oil (walnut, sesame, almond) to avoid oxidizing it and making it inflammatory.
Fats are also recommended to be spread out throughout the day, and servings can look like:
1 TBSP olive oil: 120 kcal, 13 g fat
100 g avocado: 167 kcal, 15g fat
4 oz. Spanish sardines: 290 kcal, 20g fat, 24g protein
1 oz. (28) walnuts: 190 kcal, 18g fat
1 TBSP coconut manna: 100 kcal, 9g fat
3 oz. Camembert cheese: 255 kcal, 21g fat
Carbohydrates

Let's be clear when I say carbohydrates: I do not mean carbs from corn flakes, granola bars, pasta, white flour products, or Wonder Bread. I could write a whole blog post poking holes in white flour alone, but my intent is not to demonize foods—it's to highlight the ones that will keep you healthy in your future years! These carbohydrate sources come from fibrous green and leafy vegetables, root vegetables, squashes, starchy tubers, and vitamins and mineral-rich fruits.
While carbohydrates in their whole and unprocessed forms are much better than in their processed and industrialized forms, I rarely see a benefit in carbohydrate intakes greater than thirty to forty percent of total calories for the sake of blood sugar control. However, this can vary based on how your body responds! If you can recall, I mentioned previous basic recommendations of:
1,600 kcal (25% protein, 30-50% fat: 480-800 kcal) for female seniors, leaving us with 25-45% of calories from carbs (400-720 kcal)
2,000 kcal for male seniors (25% protein:400 kcal, 30-50% fat: 600-1000kcal), leaving us with 25-45% of calories from carbs (500-900 kcal)
I will reiterate what I said when we talked about fats: use carbohydrates and fats as levers to fill the energy demands left when protein needs are filled. You or your family member you're helping out with diet may realize they feel much better and more cognitively present when their fats intake increases. They may also find that they feel better with more than twenty-five percent of total calories from protein. Nutrition is highly bio-individual and personal to every person, so I also think USDA recommendations are completely B.S.!
When consuming carbohydrates, consider reaching for those that are not simple sugars. Instead, grab for carb sources that contain starch and fiber digest so that they more slowly. As a result, they do not contribute to such rapid increases in blood sugar. The types of carbohydrates not only can control blood sugar, but they also can help produce healthy bowel movements that many seniors struggle to have! I often wonder--well, not often, this isn't something that keeps me up at night--if the reason Metamucil and Benefiber took off is because of the rich of low-fiber diets rich in processed grains!
Ideas of carbohydrates fluctuate greatly depending on what you're getting. I'm not a fan of counting calories but would recommend aiming to get at least 3-5 (shooting for 5) one-cup servings of varying fruits or vegetables per day. This could look like this:
A one-cup mix of carrots, potatoes, celeriac, onion, and celery in a beef stew at dinner: 200 kcal, 2.5 g fiber
One cup of Steamed broccoli, Brussel sprouts, carrots, and peas: 60kcal, 2.8 g fiber
One cup of sautéed mushrooms and onions: 35 kcal, 2.5g fiber
125 g banana, 125 g apple: 175 kcal, 6.5 g fiber
One cup of pineapple - 82kcal, 3.5g fiber
Dairy

While USDA recommendations for seniors and the youth tend to lay low on protein recommendations, I at least give them some credit (more like the benefit of MUCH doubt) for recommending some dairy. However, it's often the low-fat type. While the "Got Milk" campaign has dropped off, I believe that high-quality, grass-fed dairy from goat, sheep, or cow can benefit those 60+ for its contents in multiple minerals. Dairy is one food group I've come to see as a "superfood." Acai, cacao, goji, and other unspellable "superfoods" have nothing on dairy, as it has perfect proportions of macronutrients like carbs, protein, and fat with a high content of micronutrients.
Dairy and dairy products also contain a complex of other vitamins and minerals, like phosphorus, magnesium, iodine, fat-soluble vitamins like A, D, and K, and B vitamins, specifically B12 and B2. Fruits and vegetables do contain some calcium, but studies have shown it can be hard to absorb because of nutrients like oxalate and phytates that hinder the absorption of minerals like calcium and zinc [source]. As a result, it can be hard to get calcium from plants alone.
Industrialized dairy that produces highly homogenized and processed milk products have given the dairy industry a bad name for its effects on health and the poor treatment of animals. However, regeneratively farmed and pastured dairy is something that can give back to the environment and can help keep you healthy! I recommend looking to local, pasture-raised dairy producers that can be found on realmilk.com. Know your farmer, know how they produce your product, and understand what you're supporting.
I would recommend 2-3 servings of high-quality cow, sheep, or goat dairy. This could look like this:
1 cup goat milk: 150 kcal, 13g carbs, 7g fat, 8g protein, 250g calcium
100g feta cheese: 264 kcal, 4g carbs, 21g fat, 14g protein, 500g calcium
100g goat kefir: 59 kcal, 4.5g carbs, 3.3g fat, 2.9g protein, 170g calcium
100g sheep milk yogurt: 129 kcal, 4.8g carbs, 10g fat, 5.1g protein, 150g calcium
Concerning fermented dairy, this is a bonus for health as it contains probiotics. This can help to rebalance the microbiome and promote gut health. You can read a little bit more about the importance of a healthy microbiome HERE.
WHY NOT A SUPPLEMENT?
While dietary supplements can be beneficial for certain micronutrients (and even macros when talking about protein), I don't advise them to be something to rely upon. Why?
Many are poorly absorbed because they are in cheap forms.
With every action, there is a reaction. In the instance of taking a vitamin or a mineral—say a calcium supplement—we risk affecting other minerals related to it. Vitamins and minerals have antagonists and synergists. Taking very high doses of calcium, for example, can deplete magnesium and phosphorus over time.
Vitamins and minerals can alter the levels of pharmaceuticals you're taking. Some hinder absorption, some enhance it, and some change the effects of drugs to give unwarranted reactions.
Supplements cost money and don't taste good. I'm sorry. But there's nothing like a nice juicy steak with butter, roasted broccoli, mushrooms, and an excellent ol' sweet potato.
IN CONCLUSION
I genuinely believe that many disorders and health adversities that modern seniors are at risk for due to current dietary recommendations in place by our very own USDA. They're not natural, and the foods we're told to eat are not at all what we evolved to consume as hunter-gatherers. Our physiology has not changed much—if at all—since settling down as farmers approximately twelve thousand years ago to adapt to a diet that's cookie, cereal, McMuffin, and pasta-dominant. If you took anything away from this article, I hope it's that processed foods--specifically low protein foods, artificial fats, processed carbs, and synthetic foods--do not have a place in our diet!
If you're on a mission to radically improve your health as a senior or if you're hoping to boost the well-being and livelihood of a beloved senior, I hope this article has given you a sense of where to start. Begin with these basic recommendations and adapt them to your energy demands and where you or your loved one feels the best. Functional nutrition has been around for thousands of years and has helped to quell and manage many maladies. It's just what geriatrics needs!
If you're looking for more bio-individual help or guidance on a case that requires more specific recommendations, please shoot me a message! I'm happy to help.
SOURCES:
https://pubmed.ncbi.nlm.nih.gov/30143411/#:~:text=Thiamine%20deficiency%20has%20been%20suggested,and%20conduction%20defects%2C%20and%20depression.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2903787/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2464251/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6709577/
Sarcopenia https://pubmed.ncbi.nlm.nih.gov/24163319/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7054854/
https://pubmed.ncbi.nlm.nih.gov/18800291/
https://pubmed.ncbi.nlm.nih.gov/33830500/
The Big Fat Surprise, Nina Teicholz
Introduction to General, Organic and Biochemistry, 11e, Frederick Bettelheim